Hi there and welcome to post 67 of the Strength & Conditioning For Therapist blog. Slightly out of synch as last time we considered the effects of muscle weakness on all-cause mortality. Don’t worry, we’ll come back to part 2 very shortly. Here we’re considering which joint position is best for strength gain following a very interesting few conversations on Twitter. I’m going to tell you why training at long muscles lengths is a must for rehab!
The Challenges of Rehabilitation
I’ve said it many times before, those working in rehabilitation have the hardest job of all when it comes to exercise prescription and delivery. Those working in the fitness industry more often that not have at least half-motivated asymptomatic clients. In rehabilitation, not only do you have to get someone to buy-in to the process (we’ve discussed the psychology of buy-in before here and the effects of lockdown here), you have to take account of pain, clinical restrictions, hesitancy etc. This is all on top of an optimally-designed exercise intervention to elicit the right adaptations.
Adapting Exercise for Rehabilitation
So, I cover exercise design and adaptation a lot in my courses (e.g. Online S&C For Therapists; Making Sense of Muscle Power) and indeed the consideration of things like joint position. Failure to take account of the issues mentioned above risks either binning loads of exercises and sub-optimally loading patients, or inappropriately loading injured and vulnerable tissue.
Thankfully, there are many ways in which we can adapt exercise whilst still maintaining specificity. If you’re unsure what specificity is, it’s ensuring the exercise prescribed is designed to elicit the outcomes that you want (more on that here).
Your Patient is Symptomatic
What do you do if your patient / client is symptomatic during full range of movement (ROM) during heavy resistance exercise? Or indeed what happens if they’re clinically restricted from full ROM?
- Do you lower the load? – Do this and you lose the specificity (high loads are required for strength adaptation)
- Do you bin the exercise? – Do this and what do you replace it with, can you?
Change The Mode of Muscle Activation
Right, so you can’t do full ROM dynamic contractions, how about isometric? Maximal isometric contractions are a perfectly acceptable – and efficacious means to train muscle strength. And you often find a joint position that’s asymptomatic under load.
Can you go one better? Often people ask me if isometric training is only specific to the joint position, or whether mid-range is the best position. Here’s why it’s best to train at long muscle lengths if you can.
Which Joint Position Is Best For Strength Gain?
In answer to the question about which joint position is best, there are now many papers that illustrate the superiority of training at long muscle lengths. This in in contrast to the oft-held belief that training mid-range is best. Let me explain why.
Here’s a slide from one of my courses in which we explore a few ways to progress or regress resistance exercise. Remember, we’re trying to maintain specificity – so lowering the load is the last option for us.

I’ve highlighted Mode and Angle of these options as the manipulable variables that we’re focussing on and the specificity of the training/rehab is to develop muscle strength. So, we’re considering isometric contractions (mode) and we’re going to experiment with angle (to try avoid symptoms).
Is this an effective strategy? One of the key studies on this topic is by Noorkoiv et al (2015). They evaluated the effects of training the knee extensors at long vs. short muscle lengths on isometric and concentric peak torque (strength) and hypertrophy.
The participants trained for 6 weeks, 3 times per week, with 5 sets of 5 (5-s) maximal voluntary isometric contractions (MVCs) per session. 5s inter-rep rest, 1min inter-set rest. Here’s what they found:
- Concentric torque increased significantly by 12-13% after training only in LONG LENGTHS at angular velocities of 30 and 120 rad · s(-1).
- Muscle size increased in LONG LENGTHS only, the changes were correlated (r = 0.73-0.93, P < 0.05) with the changes in concentric torque.
- Isometric training-induced increases in muscle size and concentric torque were best elicited by training at LONG MUSCLE LENGTHS
Bottom line, isometric training elicited increases in muscle strength. When training occurred at long muscle lengths, increases in slow and moderate velocity concentric isokinetic torque and muscle size were also evident.
Training at Long Muscle Lengths – Isotonically
What’s really nice is that these findings also hold true for dynamic muscle contractions. I often encourage people to find a pain-free, or reduced pain ROM and lift heavy compared to reducing the load and maintaining the ROM and losing specificity. This is so nicely illustrated by Pedrosa et al (2022)
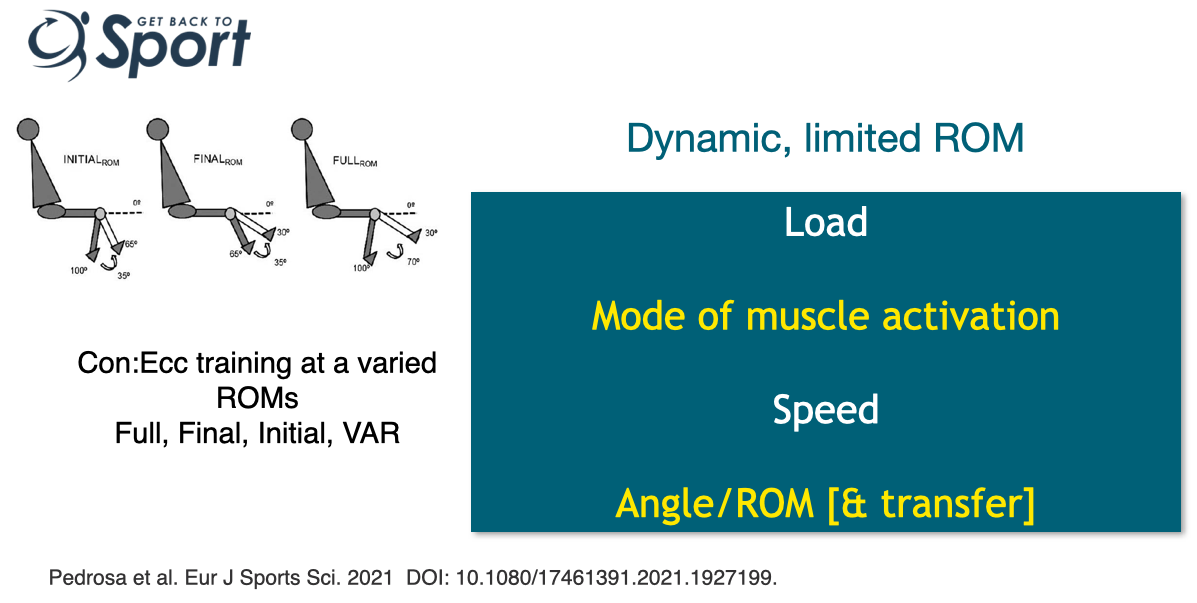
Again, they demonstrate the superiority of training at long muscle lengths – even when training through a very limited range of 35 degrees. By comparison to full range of motion (ROM) training, initial range (100 – 65 degs knee flexion) demonstrated similar strength gains assessed over a full ROM 1RM to full ROM training. Crazy, right?
Always Train at Long Muscle Lengths?
Clearly, I’m not advocating that we ditch all modes of training in favour of purely training at long muscle lengths – well at least I hope that’s clear. Nor am I trying to promote isometrics as superior to other models of exercise, far from it. The point I’m trying to make is that there are many things that we can consider changing in our exercise and rehab prescriptions before we reduce the load. If you’ve determined, high loading or training with explosive intent (read more on that here) is appropriate, but there are clinical considerations that mean that you can’t do this with full ROM for example, stop to think for a moment. Are there things about the exercise parameters that you can change, which are safe to do, but which means you can maintain the focus of the exercise?
Strength & Conditioning For Therapists
Enrolment to this S&C programme for therapists closes on 16th September 2022. We cover this and so much more on exercise adaptation, plus the fundamental concepts of S&C that you can apply to better your rehab prescriptions.
References
- Noorkoiv et al (2014). Med Sci Sports Exerc. 46(8):1525-37.
- Pedrosa at al. (2022). Eur J Sport Sci 22(8):1250-1260

