Hey there. Welcome to post 40 of Strength & Conditioning for Therapists: Is strength important in rehabilitation? Sure it is, isn’t it? This week we’re going to discuss perhaps just how important it is relative to other things. As a jobbing therapist you likely have a multitude of rehabilitation outcomes and things you need to progress with patients. Once you’ve got pain under control and your patient is emerging from the acute phase of care, how do you start to establish a hierarchy of importance of the indices of muscle function? How do you prioritise what work on and when?
Important Indices of Muscle Function
Just to clarify what I’m talking about here, broadly speaking from a muscle function or performance perspective we can develop specific rehabilitation and conditioning interventions to target muscle:
- strength
- power
- endurance
- sensori-motor performance / proprioception
Then there’s hypertrophy, and yes, plus a few other more detailed parameters.
If you’ve read any of my other posts, you’ll know about the concept of specificity and the need to have specific interventions to target specific outcomes, that is to say, you can’t expect big gains in proprioceptive acuity following a muscle endurance training programme.
Which Comes First; Muscle Endurance Or Muscle Strength?
Let’s put proprioception aside for a minute and focus on muscle resistance exercise. What do you focus on first: endurance; strength; hypertrophy, power? Hands up if you go with muscle endurance? It seems to be the typically-taught approach in therapy/rehab. In personal training, teaching is around building hypertrophy first – before strength, for what reason I’m not sure, perhaps to initiate the non-exerciser to exercise..?
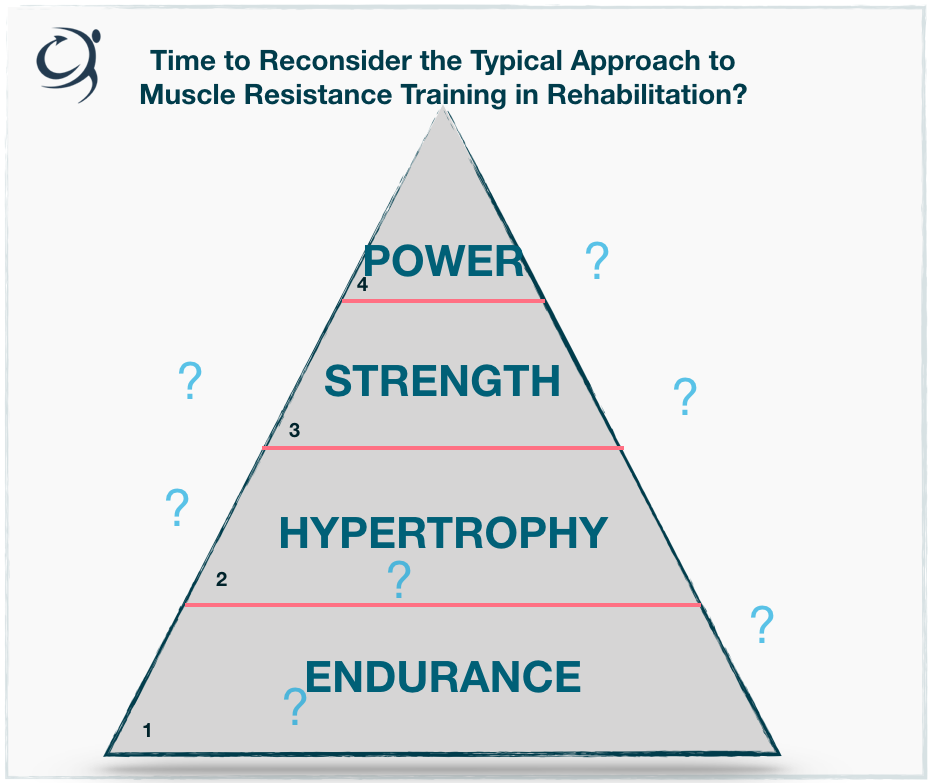
Anyways, in each and every application that I come across muscle strength appears down the list of priorities and is considered much later ‘only when…’ (that’s if it’s properly considered at all).
Strength First?
So, what I want to do here is suggest, and actually encourage, that we consider muscle strength first and foremost. Once the tissues are able to tolerate high loads (bear in mind here, this doesn’t have to be dynamic loading) and it’s clinically appropriate let’s programme for muscle strength gain in patients first.
Maybe this is a bit of a prickly idea for you. I get that, maybe it’s something you’ve not been used to doing. Heavy loading can be daunting (check out my post here on loading older populations and the ‘fragile’), but I encourage you to think about the reasons for not.
Personally I’m yet to see any scientific evidence that strength training in patient populations and in the old and the the ‘fragile’ is harmful, in fact, there’s a heap of evidence to the contrary (see link to post above). Clearly I’m not suggesting bowling on in with a voluminous 3-5RM resistance training (RT) prescription on day 1 with naive exercisers and those in considerable pain (although, this might be appropriate with a subset of those habituated to RT), but I’d argue that a progressive and individualised approach to strength training is hugely beneficial in the initial stages rehab.
Muscle Strength Is Important in Rehabilitation
I’ve written at length about what muscle strength is and why strength it’s important (for a more detailed discussion see here) but as a quick reminder, here’s a summary.
Strength Is Your Fuel Tank
Muscle strength (or maximal muscle strength, if we’re being precise) is the maximal force generating capacity of a muscle or muscle group in a single contraction.
During everyday activities, we don’t normally tend to use our full strength, thus most efforts in life and in (most) sports are sub-maximal. However, what happens if you’re weak? Consider a frail or very weak person standing up out of a chair; this could represent a near-maximal effort for some. Therefore, that person may only manage a couple of repetitions – their fuel tank is empty.
Now consider that that individual undertakes a strength training programme – tops up their tank of strength. The effort required to raise their body mass off the chair becomes considerably less; it becomes sub-maximal and thus they’re able to perform far more repetitions, with ease.
Strength is Important for Power
Power is basically the speed of muscle force production. Think about trying to develop power in a patient with this level of conditioning (above). Whilst speed of force production is important to help right posture and avoid a fall, if their fuel tank of strength is running, low, it doesn’t matter how quickly they can produce force if they don’t possess adequate force capacity to stabilise the joint(s).
Strength Is Important for Quality & Quantity of Life
I’m in danger of dominating the post here by exemplifying the importance of strength. So let me brief, there are multiple studies that show the significant relationship between strength, or lack thereof and joint pain in osteoarthritis for example and indeed a couple of recent high quality meta-analyses explaining the association of muscle weakness with all-cause mortality.
Bottom, line, it’s important and we most definitely shouldn’t overlook it in rehab, in fact let’s try and prioritise its consideration.
Strength First, then Individualise
So, I propose a revised approach to muscle resistance training in rehabilitation. Let’s build a solid foundation of muscle strength capacity first in rehabilitation and in doing so it will positively and quickly affect joint stabilisation capabilities, function, possibly pain and the extent of adaptation of other indices of function. Thereafter, we can tailor the specificity according to the individual’s needs and goals. Is this a power athlete like a hurdler, a rugby prop forward, a middle aged lady keen on returning to tennis or an elderly man with an OA knee and desires to keep active?
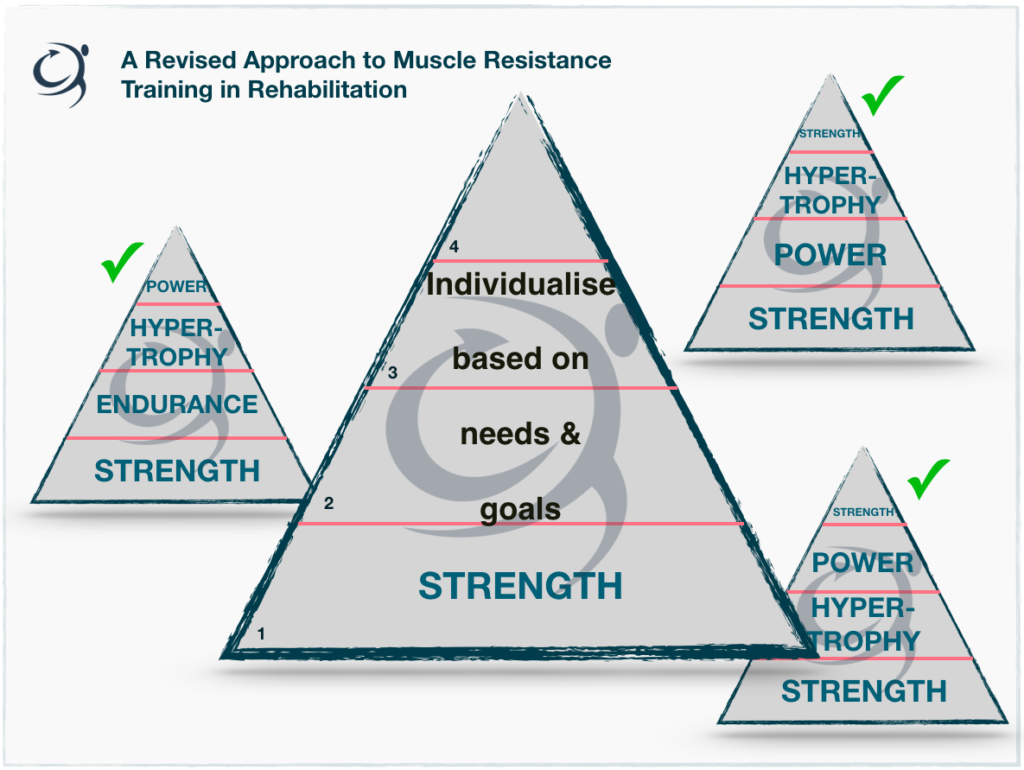
Just how long and how much (i.e. the dose) required for each aspect of muscle function will clearly differ according to the individual, and of course, it doesn’t have to involve 4 phases and all aspects of muscle function.
Rehabilitation of Multiple Outcomes
So about year ago I wrote a post on periodisation in rehabilitation and presented this figure below. It’s from a chapter I wrote for Elsevier’s new Sports Medicine text book and it show a progressive way in which to structure rehabilitation whereby you have multiple outcomes, using a periodised approach. Whilst different surgeries, patient populations and goals will each require a specific approach, this can act as a template from which you can work from.
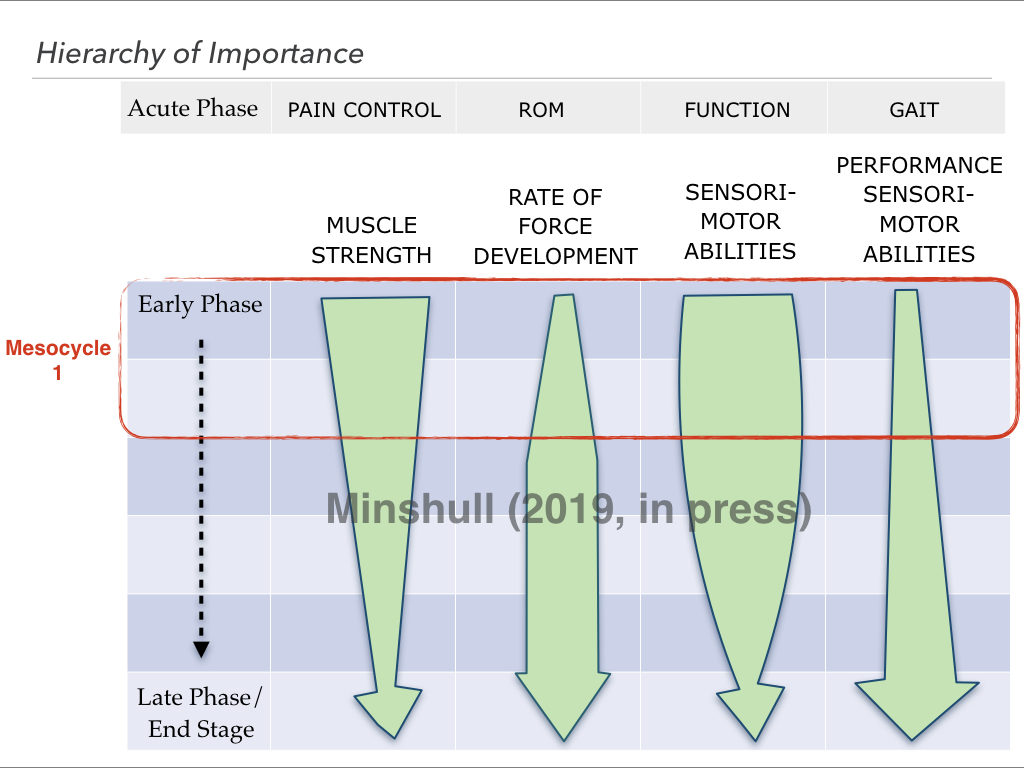
For a detailed discussion on periodisation and rehabilitation see the post here. So, in the figure above the size of the arrow indicates the focus of each phase (or cycle). Incidentally, rate of force development is the scientific equivalent of muscle power, more or less.
In column 1 you can clearly see a phased approach and tapering focus on muscle strength. In the early phase much of the focus of rehabilitation is focussed on strength – and sensory-motor abilities (proprioception), but as the programme progresses and the patient build capacity, the focus shifts on to other elements, like power and learning to utilise the newly built capacities in the specific performance settings (Performance sensor-motor abilities) .
Summary
This is a big topic and one that provokes a lot of discussion. What I wanted to achieve in this post is to prompt the reconsideration of priorities and where (if at all) muscle strength development comes in that order. I’m afraid the 3 sets of 10 with a yellow resistance band doesn’t cut it for strength development in most, nor does a set protocol or exercise sheet without individualising the approach. If we’re convinced by the evidence of the benefits of strength, or the consequences of the lack of it, then with a little thought, and a few simple tweaks to practice, we can enhance the effectiveness of our rehabilitation endeavours and our time with patients.
LOOK OUT FOR ONLINE STRENGTH & CONDITIONING TRAINING