Welcome to post 32 of Strength and Conditioning for Therapists. Following on from the last post, this week we’re going to focus a little more on the impact of muscle weakness.
What is Sarcopenia?
So mostly when people think of sarcopenia they think of it as a reduced muscle mass that is associated with ageing. Whilst is this generally accepted, a few definitions of sarcopenia exist, which vary on the extent to which they acknowledge muscle ‘quality and capability’, ie. the effects on strength and or function. Furthermore, some diagnoses of sarcopenia are applied only when there’s a failure to achieve certain predetermined scores on assessment of things such as handgrip strength and, or, walking speed. Clearly, the definition of sarcopenia will influence the prevalence statistics within a certain population. A recent systematic review and meta-analysis (ref) reported that estimates of sarcopenia prevalence in community-dwelling older adults varies from 9.9 to 40.4% depending on the definition used.
The European Working Group on Sarcopenia in Older People (EWGSOP) recently revised their definition of sarcopenia in a consensus paper. They focused on low muscle strength as a key characteristic of sarcopenia, using detection of low muscle quantity and quality to confirm the sarcopenia diagnosis, and identification of poor physical performance as indicative of severe sarcopenia. (ref). This was subsequently accepted by a number of other professional bodies: European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO), the European Society for Clinical Nutrition and Metabolism (ESPEN), International Association of Gerontology and Geriatrics European Region (IAGG-ER) and the International Osteoporosis Foundation (IOF).
So, more recent definitions of sarcopenia acknowledge much more the aspects of muscle strength (or weakness), rather than muscle volume in the diagnosis of the disease. This seems pertinent given the points I highlighted in the previous post that show that muscle strength is more strongly associated with quality and quantity of life than muscle volume.
Prevalence of Sarcopenia
Sarcopenia can affect individuals from approximately the 4th decade of life and rather alarmingly, you could expect a 30–50% decrease in skeletal muscle mass and function by the time you get to 80 years of age (ref) and power declines at a rate of 3–4% per year in older people. Now clearly, loss mass and function is worsened in sedentary / inactive people where there’s significantly greater unloading of muscle compared to more active individuals. So don’t panic just yet!
As highlighted above, prevalence can vary according to the definition adopted. Sarcopenia increases from 14% in those aged above 65 years but below 70, to 53% in those above 80 years of age. According to Santilli et al (2014), a conservative estimate is that prevalence of sarcopenia affects >50 million people today and will affect >200 million in the next 40 years, presumably due to population growth and our propensity to live increasingly sedentary lives.
The Cost of Sarcopenia

Right, I guess this is what caused you to click on the link and come to read this post. Why are we bothered about sarcopenia and muscle weakness? Well, in the previous post, we looked at some of the physical consequences, namely its effect on quality and quantity of life. Another consequence is the financial impact of sarcopenia and the need to provide care and treatment for people who are suffering the consequences.
Last year Pinedo‐Villanueva et al (ref) published a paper that attempted to quantify the economic costs of sarcopenia / muscle weakness in the UK by calculating the excess economic burden caused by provision of (additional) health and social care of those with and without muscle weakness.
This paper drew from data of The Hertfordshire Cohort Study (HCS), which comprises of 1579 men and 1418 women who were born in Hertfordshire in 1931–1939 and who still lived there in 1998–2004 and the sample for these analyses were 442 participants (221 men and 221 women) who had the full compliment of data sets. You can read more about this cohort in the paper.
The authors defined muscle weakness (N = 49) by low grip strength: men < 26 kg, women < 16 kg (Foundation for the National Institutes of Health Sarcopenia Project) and used standardised unit costs for each element of care provided. Take a look at the table below to see how things shaped up.
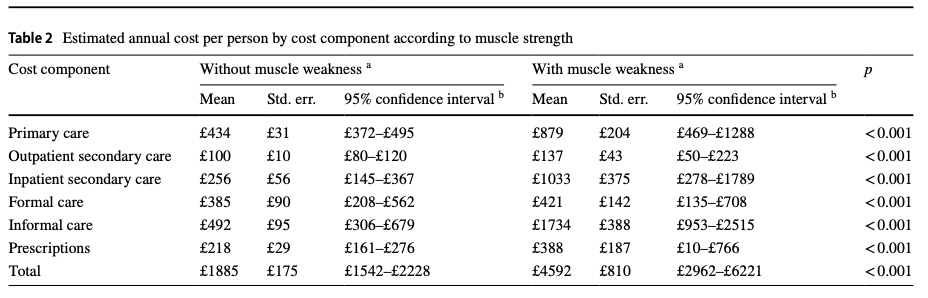
Among HCS participants, the excess economic burden associated with muscle weakness was estimated to be £2707 per person per year (£4592-£1885), with informal care and inpatient secondary care accounting for 38% and 23% of the total excess costs, respectively.
So, how did they get to the £2.5 billion per year cost? Well, they used UK population data, which estimated in 2016 the population of people aged 70 years and older was 8.2 million; they assumed that the prevalence of muscle weakness in the UK population was similar to the cohort analysed in the study (11.1%) and then multiplied that number of people by the per person per year excess cost of £2707 for muscle weakness. This results in an annual excess cost associated with muscle weakness of a whopping £2.5 billion per year.
Yes, there are clearly limitations associated with this study, including: the authors make a lot of assumptions in extrapolating their case data to a whole population, there’s likely a responder bias in the study (those perhaps with more positive/healthy behaviours are more likely to consent to be involved in the study) and there are likely some who would argue that their criteria for muscle weakness isn’t the best/preferred. However, this is a really good paper and it provides a credible estimate of the costs of muscle weakness.
I know prevention is so difficult to sell, but maybe this might just add a little more urgency to the argument to policy makers and funders to support ‘exercise- & strength-based’ projects with a slightly longer term view, especially where there’s a desperate need to create efficiencies and save money. I speak from experience and the frustrations of providing a commissionable and cost saving solution to this but that seemingly presents a too big a challenge to the politics of ‘what’s gone before’.
At the time of writing this, we’re in the 4th week of my Online course: Strength & Conditioning for Therapists. 100 Therapists from 10 different countries are going through this implementation programme, with some amazing results and fabulous feedback! If you’d like to be first to know about the March 2020 enrolment, click the link below and I’ll make sure we do just that!