Welcome to post 42 of Strength & Conditioning for Therapists.
I recently got into a discussion on Twitter about measurement, specifically, measuring strength with hand held dynamometry – is it worth doing in patients and if so how to do it…or something like that anyway. It’s difficult to convey any degree of detail or meaning in a series of tweets, so I thought I’d write a post on it. Hand held dynamometer (HHDs) can give great information on muscle strength, BUT, we need to understand the measurement limitations before we dive in.
Is Hand Held Dynamometry Useful?
Handheld dynamometers have meant that instead of buying large and expensive machines, we can relatively easily and cheaply assess muscle performance in clinic settings. I say relatively cheaply, it’s still £400 – £1000 for this kit but it’s not the prohibitively price tag of over £10,000 for isokinetic dynamometry
I think the more important question is not if HHD is useful, but do you understand the limitations of the equipment that you’re using? And importantly do you use standardised repeatable protocols to maximise the utility of these measures? Then we can ascertain if it’s useful? Let me explain.
Measuring Muscle Strength
First off, let’s consider the measurement. Generally you want your patient to push or pull against something, typically that doesn’t move and then get a a reading in meaningful units, like Newtons or kilograms. It’s not magic or wizardry, there’s a complex series of events happening.
Several dynamometers have a strain gauge set-up; very fine wire that deforms when you apply a force to it. This causes a change in electric resistance and these units are used to calculate the ‘force’ output. Importantly, in order for the units of measurement to have any usefulness at all the change in resistance should be linear when strain (/force) is applied. Indeed this linear relationship is required for all types of force assessment in this way.
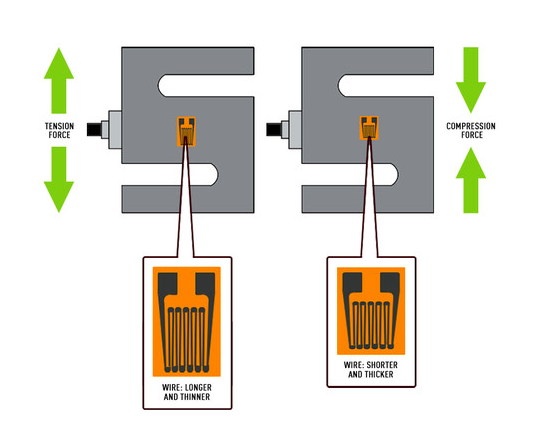
A basic example, apply exactly 5kgs of strain to the gauge and you get a measurement or reading. If the relationship is linear, place 10kgs of strain on the dynamometer and you should produce a reading of roughly double; 15kgs should be triple etc… All measurements involve some degree of error, but the key is to ensure the level of error is minimal.
What is Measurement Error?
When we’re thinking about measuring strength with hand held dynamometry – well any measurements really, we need to understand error. Broadly speaking the errors in measurements come from technical and biological sources. Through our testing protocols we need to minimise the intrusion of these errors such that we can be confident that the figures we’re seeing for strength assessment, for example, are ‘real’.
Technical Error:
This refers to the variability of the equipment (we want consistency not variability). For example, if you hang exactly 10kgs off the strain gauge several times, you get the same reading each time; well almost, there’s likely to be just a tiny difference. If there’s a big difference, throw your device in the bin! Or consider your test set up…
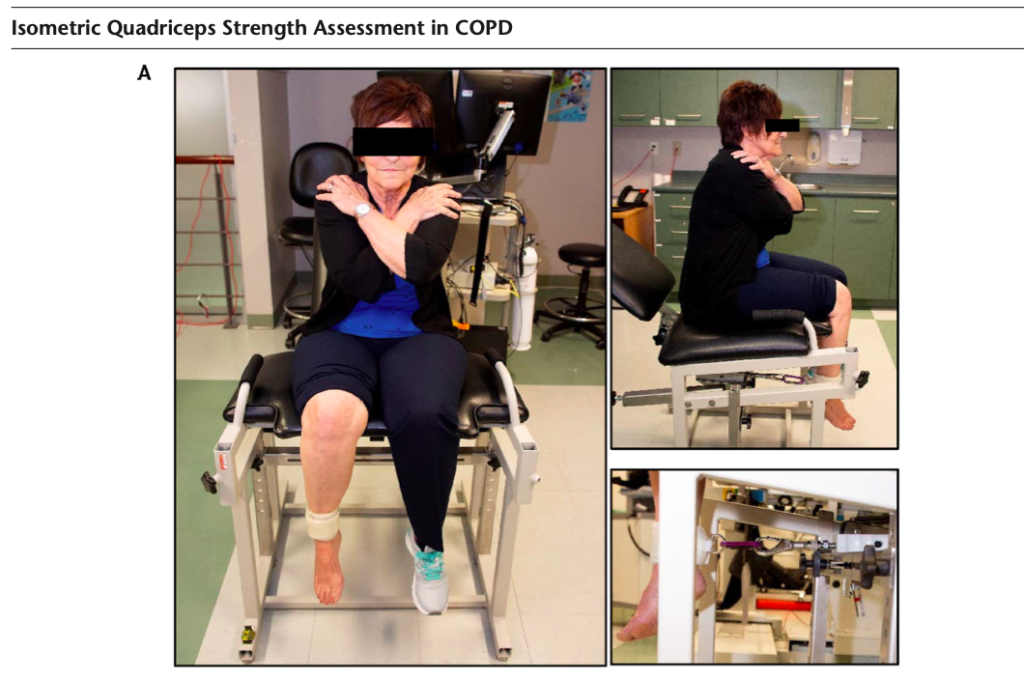
Technical error also refers to the variability in measures coming from the protocol or set-up. Here we’re trying to minimise any extraneous movement and test set-up differences that will change the strain applied to the gauge and lead to a misinterpretation of the data. Think about the difference of tethering a HHD to an immovable pice of apparatus. Having the patient secured and appropriately tethered into a seat and getting them to push against it, versus you holding the HHD and applying the resistive force and the patient sliding all over the place. The latter involves a lot more variability, or error that will intrude into the measurement, possibly rendering any it useless. See below for a good example of measuring strength using hand held dynamometry, minimising technical error.
Biological Error:
This refers to the variability of ‘the person’. On repeated tests, using the exact same set-up, how much does a person’s measurement of strength vary by? People are naturally variable. Even on repeated strength assessments separated by just a couple of minutes, there’ll be a small difference in strength between measure 1, 2, 3 etc. But, if this person is familiarised to the test, they’ve practiced enough to be consistent and of course they’re asymptomatic, this biological variability should be very little.
Hand Held Dynamometry; Minimising Error
So, when you get your HHD out of the box, think carefully about how you’re going to use it and think about how you’e going to minimise the technical and biological error. Here are some pointers to start with:
- Firstly, standardise the test set-up. To make meaningful comparisons between and within people, you need to follow the exact same procedure each and every time.
- Minimise the technical variability by securing the HHD to something that doesn’t move if possible, the could even be the leg of the stool a patient is sitting on. Standardise the patient positioning and minimise any unwanted movement, strapping may be required.
- Standardise the placement of the HHD on the limb – how far relative to bony landmarks etc. For thigh muscle testing this might be 1 inch proximal to the lateral malleolus for example.
- Minimise the biological error by performing a standardised warm-up. How many sub-maximal attempt will you give each patient?
- Ensure patients are familiarised and habituated to the test. Does the patient understand exactly what you want them to do? i.e “push against this hard” vs. “push against this as hard and as fast as you can until I say stop” Several practice attempts will help minimise ‘false’ improvements in scores. due to learning (ensure sufficient rest is given!)
- Know how many efforts are you going to record Will you take the best attempt, or the mean or three, say?
These are just a few really important considerations that you need to think about before you even switch your device on. Once you’ve established your protocol/s, you can then start to evaluate the test sensitivity or accuracy. But I think that’s enough for now. Next time I’ll show you a protocol to follow for HHD and how to evaluate the accuracy of your in-clinic measurements.



