Welcome to week 13 of the S&C for Therapists blog. 🙂
These past few weeks I’ve been writing and producing a webinar for the great David Pope and his Clinical Edge platform (very honoured!). Something that I covered, and which cropped up in the Twitter questions to me a couple of months ago was to do with compound versus isolation exercises. Which is best for rehab…? So I’m going to cover that a little today, from a basic perspective and then in a future post we’ll see if either performs superiorly in rehab.
What’s The Difference Between Compound & Isolation Exercises?
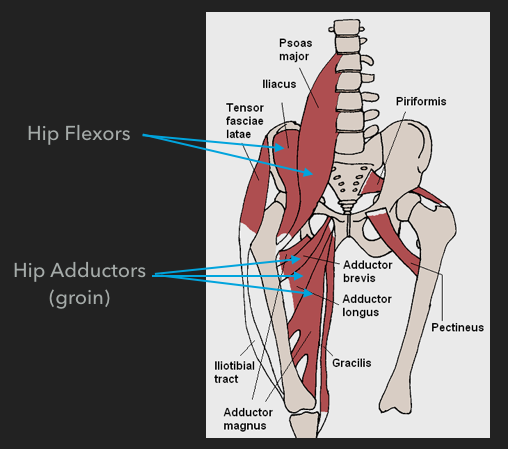
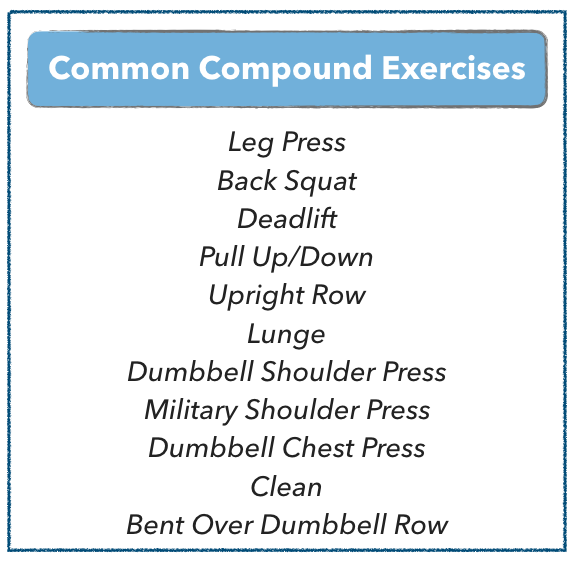
Compound exercises are those that work multiple muscle groups at the same time, often over multiple joints. A typical example of a compound exercise would be a squat. This exercise requires activation of the quadriceps, glutes, hamstrings, and calfs to bring about (or control) motion at the hips knees and ankles.

Other compound exercises include:
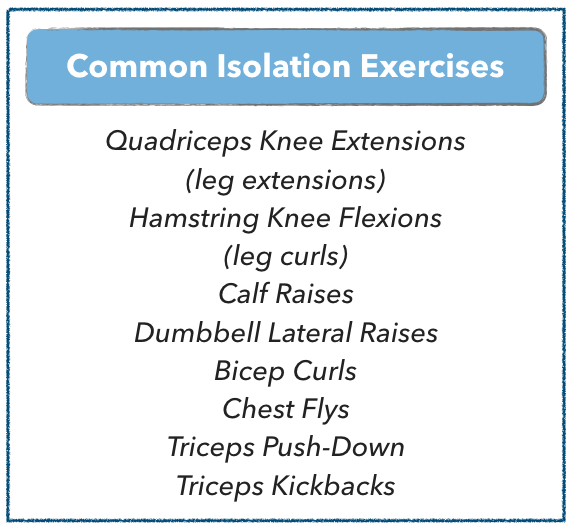
Isolation exercises, as the name suggests, isolates the musculature that controls motion about a single joint. An example of an isolation exercise is a biceps curl, especially if the shoulder joint is stabilised.

Other isolation exercises include:
Compound Or Isolation Exercises For Rehabilitation?
Obviously, I’m going to say ‘it depends’ here aren’t I? Tut. Both compound and isolation exercises have their merits and challenges and during exercise selection we need to take account of some key things, which include:
- Injury status
- Goals of the rehab
- Phase of the rehab
- Goals of the patient
- Patient exercise experience
In my opinion, as long as you properly take account of these things you can build a rehab program that uses both types of exercises for any phase of rehab and for most patient profiles. Before we exemplify, I’ve noted below a few of my thoughts about the merits and challenges of compound and isolation exercises.
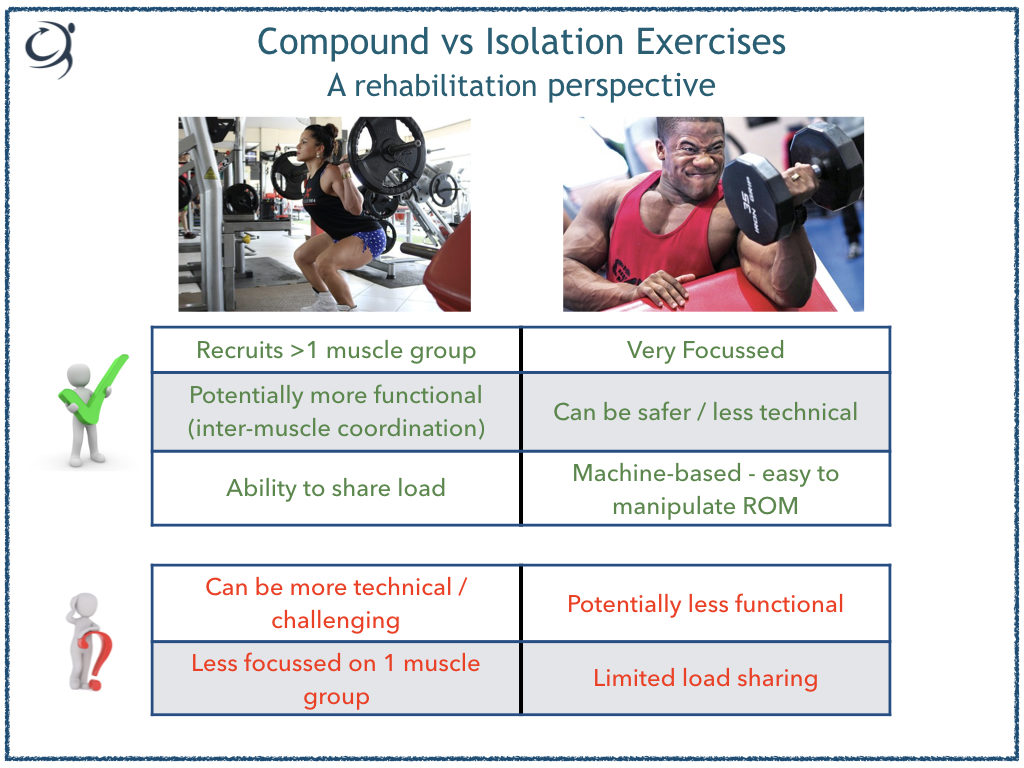
Advantages of Isolation Exercises
I know a lot of people don’t like isolation exercises and Functional Training or Functional Rehab is all the rage. Functional Training has its place, don’t get me wrong, but if we blinker our approach too much, we might not get the gains in our patients that we’re hoping for.
For me, a key advantage of isolation exercises is that you can hone your focus on a particular muscle group. With machine-based exercise especially, you can really load up that muscle group safely. For example, the knee extension machine is a fantastic tool to isolate the quadriceps to build strength. As we know, high load and few repetitions are required to optimally build strength (see here on how to train strength). Whilst a criticism of the knee extension is that it’s not very functional, in the early phases of rehab and, or, with patients that are inexperienced resistance trainers it’s a much safer alternative for strength building than a back squat for example and can be fantastically effective. Once the patient has developed adequate strength, whatever you dee that to be, you can then start to think about loading in a more functional way.
Advantages of Compound Exercises
Clearly compound exercises that involve multiple joints can be more functional and help to develop inter-muscular co-ordination. Fine. But these exercises can be fairly technical and require a certain level of competency before we can start to load them up to develop strength. That doesn’t necessarily mean you have to omit them from early phase rehab. For me an additional advantage is that you can load-share between limbs. Let’s take a leg press for example in a patient with OA knee pain.
First, the leg press is a nice progression from a knee extension to build to a squat, but with OA knee pain, closed kinetic chain (where the foot is in contact with the floor/a solid surface) strength training might provoke pain in deep flexion. Okay, so instead of using this as a strength exercise straight away, we can use it as a ‘functional’ exercise that familiarises the person/joint to accommodate load during closed-kinetic chain positions. The non-painful limb can modulate the load taken by the painful limb during the deeper and more painful ranges of motion.
We might also want to consider doing upper body work too. A landmine press incorporating a squat can also be a good progression from the above
See link here for example of a landmine press You can play around with the depth of squat according to patient symptoms.
Summary
So, compound vs isolation, which is best..? Both are good and I’d encourage you to use both types in your rehab and conditioning. It might be in the earl phases of a programme with an inexperienced patient, isolation exercises present the best way to develop pure strength (3-5 RM), but sub-maximal compound exercises can be performed concurrently with the goal of developing technique and load tolerance.
COMING VERY SOON…..!
Please click below if you’d like to be notified directly about the DOWNLOAD that covers how to tailor your resistance training with patients to achieve specific goals and of the WEBINAR for a more in-depth look at this topic please pop your name and email below and I’ll send you notification straight into your inbox.